Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 07/01/2024 - 06/30/2025
State of Illinois: State Plan Coverage for: Individual + Family | Plan Type: HMO
The Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the
plan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be
provided separately. This is only a summary For more information about your coverage, or to get a copy of the complete terms of coverage,
www.healthalliance.org/stateofillinois or call 1-800-851-3379. For general definitions of common terms, such as allowed amount, balance billing,
coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at
https://www.healthalliance.org/documents/1492 or call 1-800-851-3379 to request a copy.
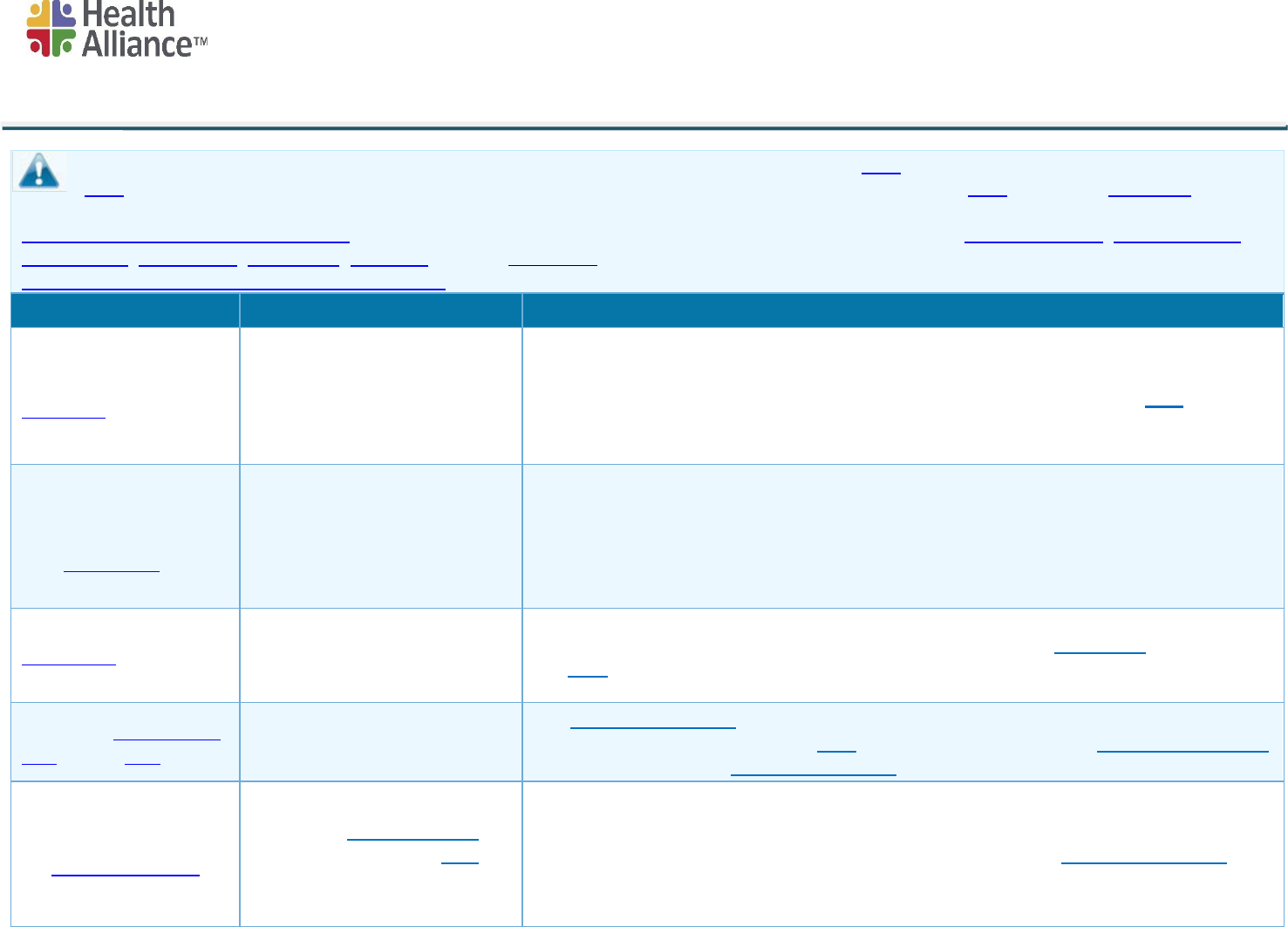
Important Questions
Answers
Why This Matters:
What is the overall
deductible?
$0
See the Common Medical Events chart below for your costs for services this plan covers.
Are there services
covered before you meet
your deductible?
No.
Are there other
deductibles f
or specific
services?
Yes; $150 Prescription Drugs
You mu
st pay all of the costs for these services up to the specific deductible amount before
this plan begins to pay for these services.
What is the out-of-pocket
limit for this plan?
$3,000 Individual/ $6,000
Family
The out-of-pocket limit is the most you could pay in a year for covered services. If you
have other family members in this plan, they have to meet their own out-of-pocket limits
until the overall family out-of-pocket limit has been met.
What is not included in
the out-of-pocket limit?
Premiums, balance billing
charges, healthcare this plan
does not cover.
Even though you pay these expenses, they don’t count toward the out–of–pocket limit.
1 of 9
* For more information about limitations and exceptions, see the plan or policy document at www.healthalliance.org/stateofillinois.
2 of 9
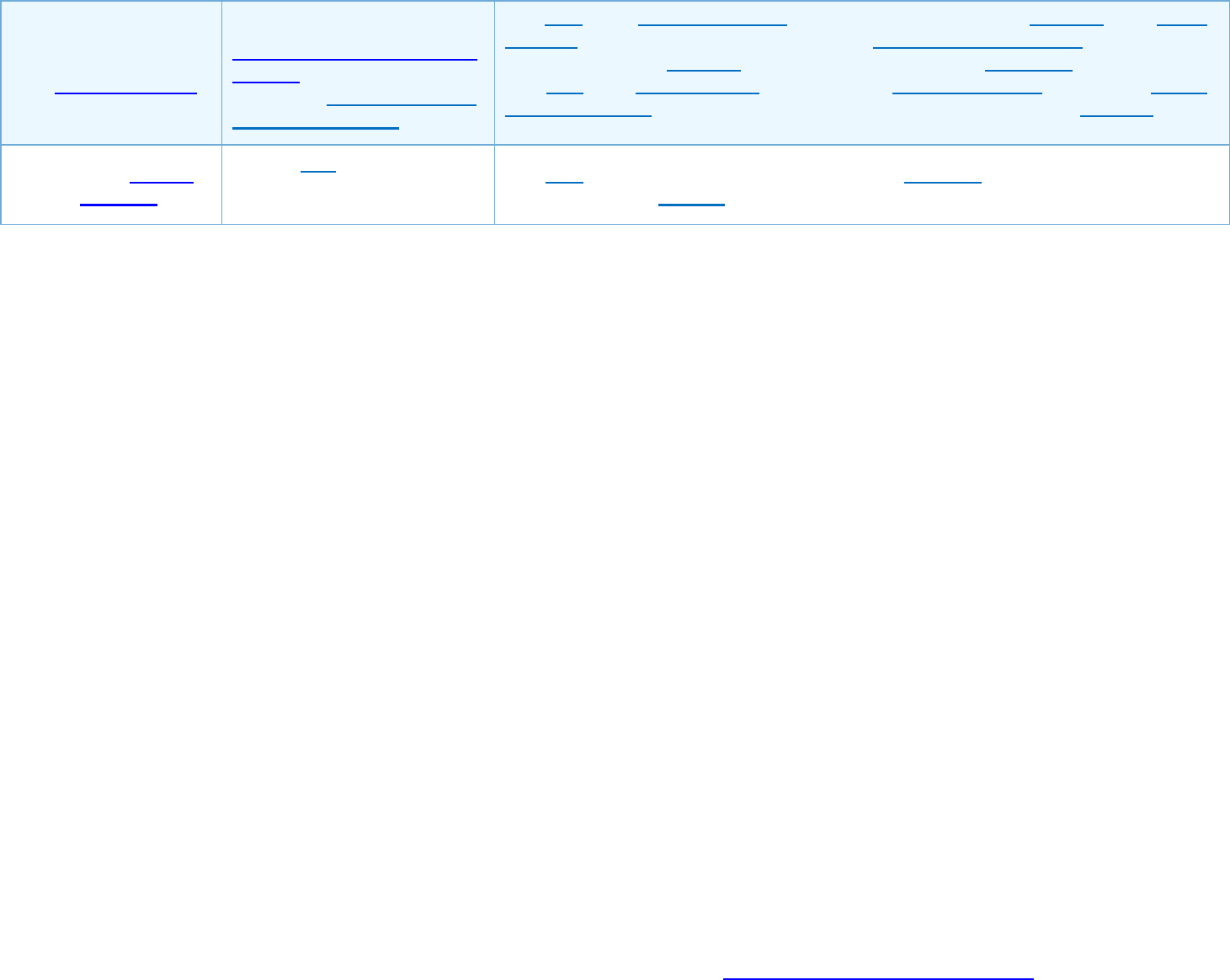
Will you pay less if you
use a network provider?
Yes. See:
www.healthalliance.org/state
ofillinois or call 1-800-851-3379
for a list of Participating (In-
network) providers.
This plan uses a provider network. You will pay less if you use a provider in the plan’s
network. You will pay the most if you use an out-of-network provider, and you might
receive a bill from a provider for the difference between the provider’s charge and what
your plan pays (balance billing). Be aware your network provider might use an out-of-
network provider for some services (such as lab work). Check with your provider before
you get services.
Do you need a referral
to see a specialist?
Yes, this plan may require
referrals to in-network
specialists.
This p
lan will pay some or all of the costs to see a specialist for covered services but
only if you have a referral before you see the specialist.
* For more information about limitations and exceptions, see the plan or policy document at www.healthalliance.org/stateofillinois.
3 of 9
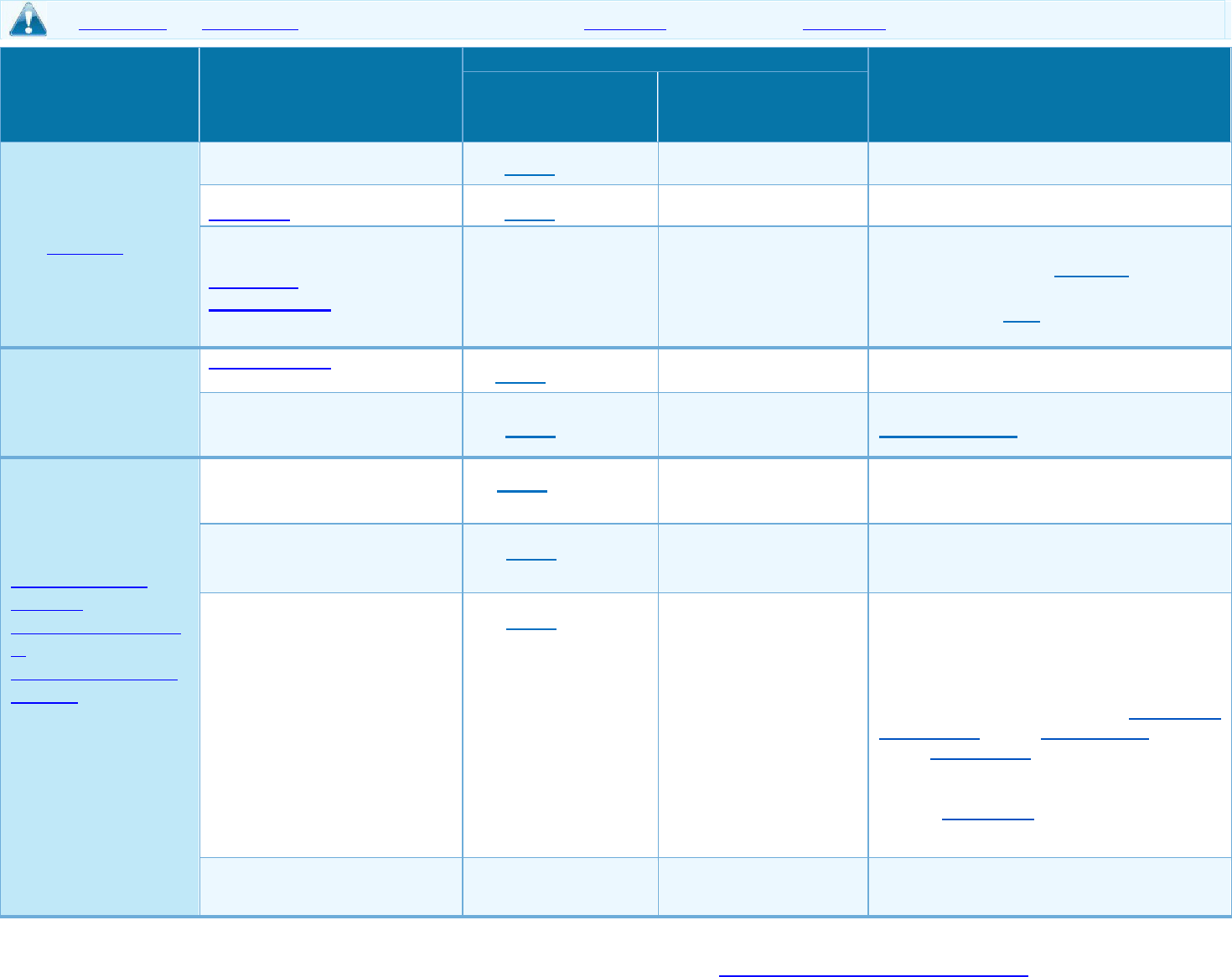
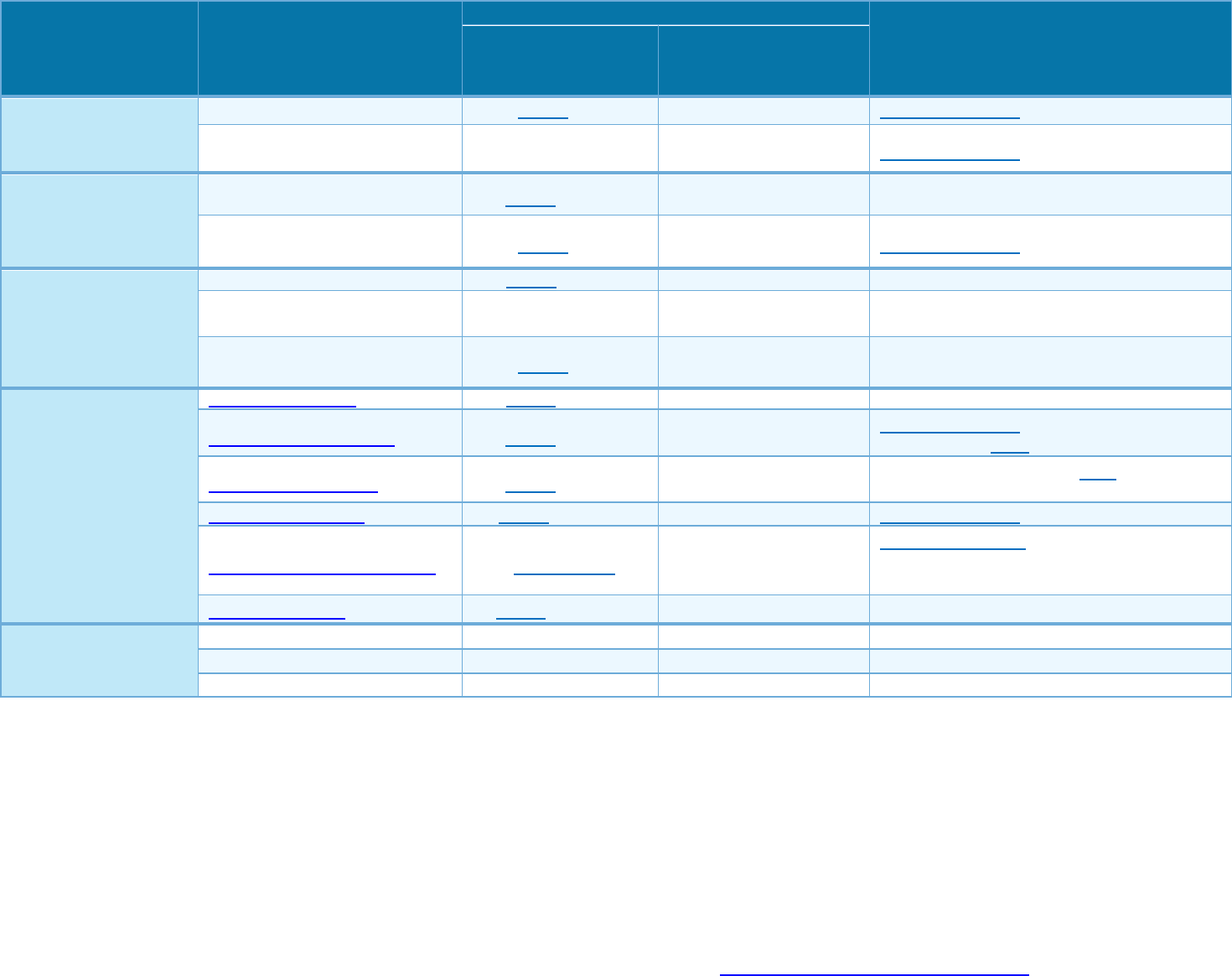
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other Important
Information
Participating (In-
Network) Provider
(You will pay the least)
Non-Participating (Out
of Network) Provider
(You will pay the most)
If you visit a health
care provider’s office
or clinic
Primary care visit to treat an
injury or illness
$30 copay/visit Not Covered --none--
Specialist visit $40 copay/visit Not Covered --none--
Preventive
care/screening/
immunization
No Charge
Not Covered
You may have to pay for services that aren’t
preventive. Ask your provider if the
services you need are preventive. Then
check what you plan will pay for. Refer to
Wellness Brochure.
If you have a test
Diagnostic test (x-ray, blood
work)
$0 copay/service Not Covered --none--
Imaging (CT/PET scans,
MRIs)
$30 copay/service Not Covered Preauthorization Required
If you need drugs to
treat your illness or
condition
More information about
prescription drug
coverage is available at
https://healthalliance.o
rg
/documents/formulary/
661/2024
Reduced Generic Tier 1
$4 copay /
prescription
Not Covered
Covers up to a 30-day supply (retail
prescription); 90 day supply (mail order)
available for 2.5 copays.
Generic Tier 1
$20 copay /
prescription
Not Covered
Covers up to a 30-day supply (retail
prescription); 90 day supply (mail order)
available for 2.5 copays.
Preferred Brand -
Preferred Specialty Tier 2
$35 copay /
prescription
Not Covered
Covers up to a 30-day supply (retail
prescription); 90 day supply (mail order)
available for 2.5 copays. If you or your
Physician requests a brand name drug
when
a generic drug exists, you pay the
Preferred
Brand or Non-Preferred Brand Deductible
,
Copayment and/or Coinsurance, plus a
100% coinsurance for the difference in
cost
between the Brand name drug and the
Generic drug. This price difference is
applied
to your Deductible. In no instance will the
total cost you are charged for the drug
exceed the actual cost of the drug.
* For more information about limitations and exceptions, see the plan or policy document at www.healthalliance.org/stateofillinois.
4 of 9
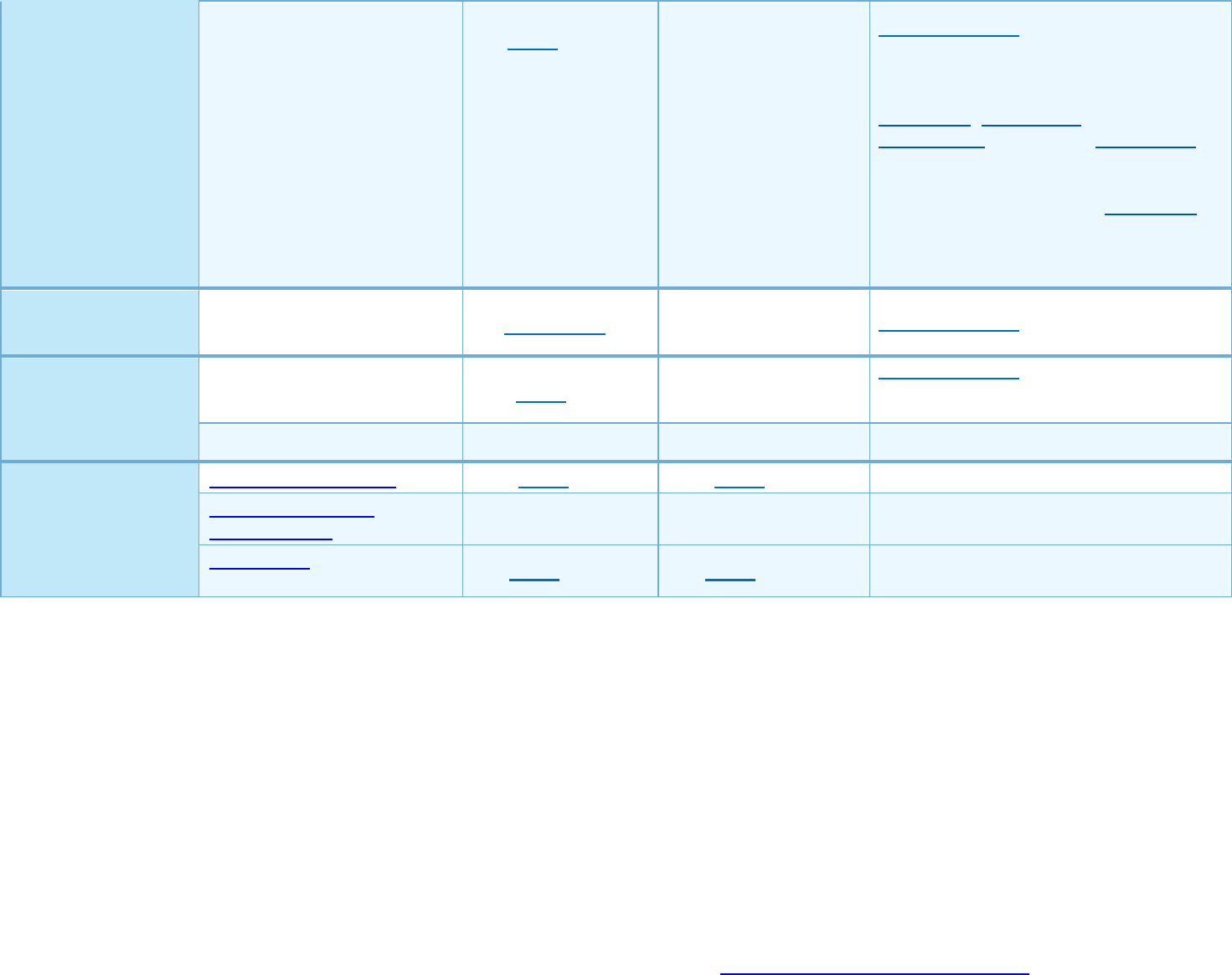
Non-Preferred Brand -
Non-Preferred Specialty Tier 3
$60 copay /
prescription
Not Covered
Preauthorization may be required. If you or
your Physician requests a brand name drug
when a generic drug exists, you pay the
Preferred Brand or Non-Preferred Brand
Deductible, Copayment and/or
Coinsurance, plus a 100% coinsurance for
the difference in cost between the Brand
name drug and the Generic drug. This price
difference is applied to your Deductible. In
no instance will the total cost you are
charged for the drug exceed the actual cost
of the drug.
Medical Drugs
0% coinsurance Not Covered
Preauthorization is required
If you have outpatient
surgery
Facility fee (e.g., ambulatory
surgery center)
$300 copay/procedure Not Covered
Preauthorization may be required for
certain procedures. Contact customer
Service for detailed information.
Physician/surgeon fees No Charge Not Covered --none--
If you need immediate
medical attention
Emergency room care
$275 copay / visit
$275 copay / visit
Participating Benefit Applies
Emergency medical
transportation
No Charge No Charge Participating Benefit Applies
Urgent care
$30 copay / visit $30 copay / visit --none--
* For more information about limitations and exceptions, see the plan or policy document at www.healthalliance.org/stateofillinois.
5 of 9
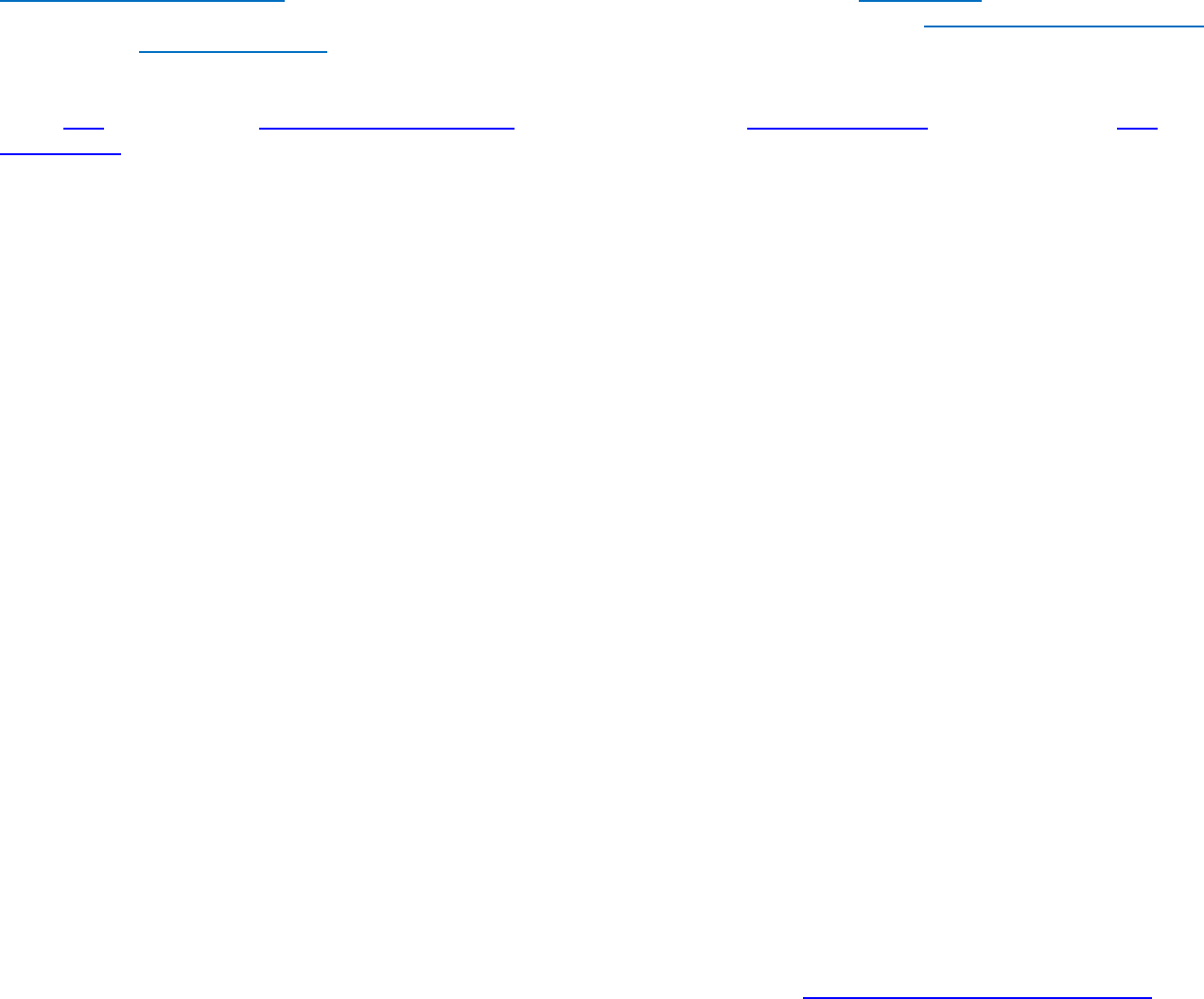
Common
Medical Event
Services You May Need
What You Will Pay
Limitations, Exceptions, & Other Important
Information
Participating (In-
Network) Provider
(You will pay the least)
Non-Participating (Out
of Network) Provider
(You will pay the most)
If you have a hospital
stay
Facility
fee
(e.g.,
hospital
room)
$425 copay / stay
Not Covered
Preauthorization is required.
Physician/surgeon fees No Charge Not Covered Preauthorization may be required.
If you need mental
health, behavioral
health, or substance
abuse services
Outpatient services $30 copay/visit Not Covered --none--
Inpatient services $425 copay / stay Not Covered Preauthorization is required.
If you are pregnant
Office visits
$50 copay/pregnancy
Not Covered
--none--
Childbirth/delivery
professional services
No Charge Not Covered --none--
Childbirth/delivery facility
services
$425 copay / stay Not Covered --none--
If you need help
recovering or have other
special health needs
Home health care
$40 copay/visit
Not Covered
--none--
Rehabilitation services $40 copay/visit Not Covered
Preauthorization is required. 60 visits per
condition per plan year maximum.
Habilitation services $40 copay/visit Not Covered
60 visits per condition per plan year
maximum.
Skilled
nursing
care
$0 copay / stay
Not Covered
Preauthorization is required.
Durable medical equipment 20% coinsurance Not Covered
Preauthorization may be required for
certain medical equipment. Contact
Customer Service for detailed information.
Hospice services
$0 copay
Not Covered
--none--
If your child needs
dental or eye care
Children’s
eye
exam
Not Covered
Not Covered
--none--
Children’s
glasses
Not Covered
Not Covered
--none--
Children’s dental check-up
Not Covered
Not Covered
--none--

* For more information about limitations and exceptions, see the plan or policy document at www.healthalliance.org/stateofillinois.
6 of 9
Excluded Services & Other Covered Services:
Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.)
• Dental Care
• Long Term Care
• Non-Emergency Care When
Traveling Outside the U.S.
• Weight Loss Programs
Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.)
• Acupuncture
• Bariatric Surgery
• Chiropractic
• Hearing Aids
• Infertility Services
• Private Duty Nursing
• Elective Abortion
Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information
for those agencies is: For group health coverage subject to ERISA, Department of Labor’s Employee Benefits Security Administration at 1-866-
444-EBSA (3272) or www.dol.gov/ebsa/healthreform.
For non-federal governmental group health plans, Department of Health and Human
Services, Center for Consumer Information and Insurance Oversight, at 1-877-267-2323 x61565 or www.cciio.cms.gov. Church plans are not
covered by the Federal COBRA continuation coverage rules. If the coverage is insured, individuals should contact their State insurance regulator
regarding their possible rights to continuation coverage under State law.
Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For
more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.
Your Grievance and Appeals Rights:
There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal.
For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also
provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights,
this notice, or assistance, contact:
For non-federal governmental group health plans and church plans that are group health plans, contact Health Alliance at 1-800-851-3379 and
State of Illinois Department of Insurance at 1-877-527-9431 or consumer_complaints@ins.state.il.us.
Additionally, a consumer assistance program can help you file your appeal. Contact 1-800-851-3379. A list of states with Consumer Assistance
Programs is available at: www.dol.gov/ebsa/healthreform and http://www.cms.gov/CCIIO/Resources/Consumer-Assistance-Grants/.
* For more information about limitations and exceptions, see the plan or policy document at www.healthalliance.org/stateofillinois.
7 of 9
Does this plan provide Minimum Essential Coverage? Yes
Minimum Essential Coverage generally includes plans, health insurance available through the Marketplace or other individual market policies,
Medicare, Medicaid, CHIP, TRICARE, and certain other coverage. If you are eligible for certain types of Minimum Essential Coverage, you may not be
eligible for the premium tax credit.
Does this plan meet the Minimum Value Standards? Yes
If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan
through the
Marketplace.
Language Access Services:
Spanish (Español): Para obtener asistencia en Español, llame al 1-800-851-3379.
Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-800-851-3379.
Chinese (中文): 如果需要中文的帮助,请请打请个号请1-800-851-3379.
Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' 1-800-851-3379.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––

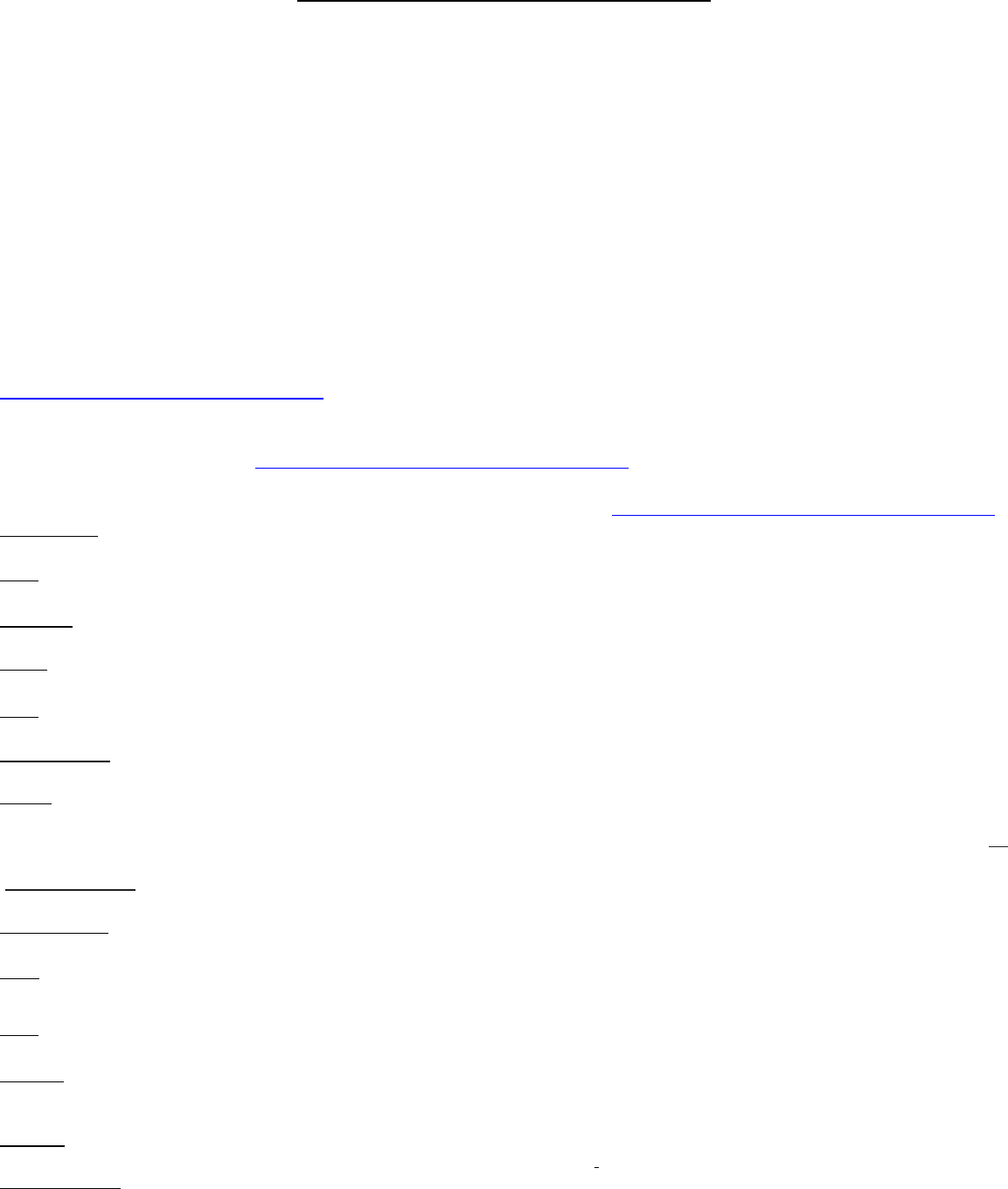
The plan would be responsible for the other costs of these EXAMPLE covered services.
8 of 9
About these Coverage
The plan’s overall deductible $0
Specialist $40 copay/visit
Hospital (facility) $425 copay/stay
Other 0% coinsurance
This EXAMPLE event includes services like:
Specialist office visits (prenatal care)
Childbirth/Delivery Professional Services
Childbirth/Delivery Facility Services
Diagnostic tests (ultrasounds and blood work)
Specialist visit (anesthesia)
Total Example Cost
$12,700
In this example, Peg would pay:
The plan’s overall deductible $0
Specialist $40 copay/visit
Hospital (facility) $425 copay/stay
Other 0% coinsurance
This EXAMPLE event includes services like:
Primary care physician office visits (including
disease education)
Diagnostic tests (bloo
d work)
Prescription drugs
Durable medical equipment (glucose meter)
Total Example Cost
$5,600
In this example, Joe would pay:
The plan’s overall deductible $0
Specialist $40 copay/visit
Hospital (facility) $425 copay/stay
Other 0% coinsurance
This EXAMPLE event includes services like:
Emergency room care (including medical
supplies)
Diagnostic test (x-ray)
Durable medical equipment (crutches)
Rehabilitation services (physical therapy)
Total Example Cost
$2,800
In this example, Mia would pay:
Mia’s Simple Fracture
(in-network emergency room visit and follow
up care)
Managing Joe’s type 2 Diabetes
(a year of routine in-network care of a well-
controlled condition)
Peg is Having a Baby
(9 months of in-network pre-natal care and a
hospital delivery)
This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be
different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing
amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of
costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.
Cost Sharing
Deductibles
$0
Copayments
$900
Coinsurance
$0
What isn’t covered
Limits or exclusions
$60
The total Peg would pay is
$960
Cost Sharing
Deductibles
$0
Copayments
$300
Coinsurance
$0
What isn’t covered
Limits or exclusions
$200
The total Joe would pay is
$500
Cost Sharing
Deductibles
$0
Copayments
$500
Coinsurance
$40
What isn’t covered
Limits or exclusions
$0
The total Mia would pay is
$540
GNCMHA24-CMnondiscrimnt-0623
DISCRIMINATION IS AGAINST THE LAW
Health Alliance
TM
complies with applicable federal civil rights laws and does not discriminate on the basis of race,
color, national origin, age, disability or sex (including pregnancy, sexual orientation or gender identity). Health
Alliance does not exclude people or treat them differently because of race, color, national origin, age, disability or sex
(including pregnancy, sexual orientation or gender identity). Health Alliance:
Provides free aids and services to people with disabilities to communicate effectively with us, such as:
Qualified sign language interpreters.
Written information in other formats (large print, audio, accessible electronic formats, other formats).
Provides free language services to people whose primary language is not English, such as:
Qualified interpreters.
Information written in other languages.
If you need these services, contact Customer Service.
If you believe that Health Alliance has failed to provide these services or discriminated in another way on the basis of
race, color, national origin, age, disability or sex (including pregnancy, sexual orientation or gender identity), you can
file a grievance with: Health Alliance, Customer Service, 3310 Fields South Drive, Champaign, IL 61822 or 411 N.
Chelan Ave., Wenatchee, WA 98801; telephone for members in Illinois, Indiana, Iowa and Ohio: (800) 851-3379,
TTY:711; members in Washington call: (877) 750-3515, TTY: 711; fax: (217) 902-9705;
CustomerService@HealthAlliance.org.
You can file a grievance in person or by mail, fax or email. If you need help
filing a grievance, Customer Service is available to help you. You can also file a civil rights complaint with the U.S.
Department of Health and Human Services, Office for Civil Rights, electronically through the Office for Civil Rights
Complaint Portal, available at
https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of
Health and Human Services, 200 Independence Avenue SW, Room 509F, HHH Building, Washington, DC 20201,
(800) 368-1019, TTY: (800) 537-7697. Complaint forms are available at
http://www.hhs.gov/ocr/office/file/index.html.
ATENCIÓN: Si habla Español, servicios de asistencia lingüística, de forma gratuita, están disponibles para usted. IA, IL, IN, OH:
Llame (800) 851-3379, WA Llame: (877) 750-3515 (TTY: 711).
注意:如果你講中文,語言協助服務,免費的,都可以給你。IA, IL, IN, OH: 呼叫 (800) 851-3379, WA: 呼叫 (877) 750-
3515(TTY: 711)。
UWAGA: Je
śli mówić Polskie, usługi pomocy języka, bezpłatnie, są dostępne dla Ciebie. IA, IL, IN, OH: Zadzwoń
(800) 851-3379, WA: Zadzwoń (877) 750-3515 (TTY: 711).
Chú ý: Nế
u bạn nói Tiếng Việt, các dịch vụ hỗ trợ ngôn ngữ, miễn phí, có sẵn cho bạn. IA, IL, IN, OH: Gọi
(800) 851-3379, WA: Gọi (877) 750-3515 (TTY: 711).
주의 : 당신이
한국어, 무료 언어 지원 서비스를 말하는 경우 사용할 수 있습니다. (800) 851-3379 IA, IL, IN, OH: 전화 WA:
(877) 750-3515 전화 (TTY: 711).
ВНИМАНИЕ: Ес
ли вы говорите русский, вставки услуги языковой помощи, бесплатно, доступны для вас. IA, IL, IN, OH:
Вызов (800) 851-3379, WA: Вызов (877) 750-3515 (TTY: 711).
Pansin: Kung magsalita ka Tagalog, mga serbisyo ng tulong sa wika, nang walang bayad, ay magagamit sa iyo. IA, IL, IN, OH:
Tumawag (800) 851-3379, WA: Tumawag (877) 750-3515 (TTY: 711).
هﺎﺒﺘﻧا:
اذإ
ﺖ ﻨ ﻛ
ﻢﻠﻜﺘﺗ
،ﺔﯿﺑﺮﻌﻟا
نﺈﻓ
تﺎﻣﺪﺧ
ةﺪﻋﺎﺴﻤﻟا
ﺔﯾﻮﻐﻠﻟا
ةﺮﻓﻮﺘﻣ
ﻚﻟ
ً
ﺎﻧﺎﺠﻣ.
،يﻮﻨﯿﻠﯾإ
،ﺎﻧﺎﯾﺪﻧإ
ﻮﯾﺎھوأ:
ﻞﺼﺗا
ﻢﻗﺮﻟﺎﺑ
3379-851
(800) ،
ﺔﯿﻟاو
ﻦﻄﻨﺷاو:
ﻞﺼﺗا
ﻢﻗﺮﻟﺎﺑ:
)711 ﻢ ﻗ ﺮ ﻟ ا ﻰﻠﻋ ﻞﺼﺗﺎﻓ ﻊ ﻤ ﺴ ﻟ ا ﻲ ﻓ ﺔﺑﻮﻌﺻ وأ ﻢﻤﺼﻟا ﻦﻣ ﻲﻧﺎﻌﺗ ﺖ ﻨ ﻛ ا ذ إ (
(877) 750-3515
Aufmerksamkeit: Wenn Sie Deutsch sprechen, Sprachassistenzdienste sind kostenlos, zur Verfügung. IA, IL, IN, OH: Anruf (800)
851-3379, WA: Anruf (877) 750-3515 (TTY: 711).
ATTENTION: Si vous parlez français, les services d'assistance linguistique, gratuitement, sont à votre disposition. IA, IL, IN,
OH: Appelez (800) 851-3379, WA: Appelez (877) 750-3515 (TTY: 711).
યાન: તમ
ે વાત તો ગુજરાતી, ભાષા સહાય સેવાઓ, મફત, તમારા માટે ઉપલધ છે. IA, IL, IN, OH: કૉલ (800) 851-3379,
WA: કૉલ (877) 750-3515 (TTY: 711).
注意:あなたは、日本語 、無料で言語支援サービスを、話す場合は、あなたに利用可能です。
(800) 851-3379 IA, IL, IN, OH: コール (877) 750-3515 WA: コール(TTY: 711)。
LET OP: Services Wann du [Deitsch (Pennsylvania German / Dutch)] schwetzscht, kannscht du mitaus Koschte ebber gricke, ass
dihr helft mit die englisch Schprooch. Ruf selli Nummer uff: IA, IL, IN, OH: Call (800) 851-3379 WA: Call (877) 750-3515
(TTY: 711).
УВАГА: Я
кщо ви говорите український, вставки послуги мовної допомоги, безкоштовно, доступні для вас. IA, IL, IN,
OH: Виклик (800) 851-3379, WA: Виклик (877) 750-3515 (TTY: 711).
ATTENZIONE: Se si p
arla italiano, servizi di assistenza linguistica, a titolo gratuito, sono a vostra disposizione. IA, IL, IN, OH:
Chiamare (800) 851-3379, WA: Chiamare (877) 750-3515 (TTY: 711).
